Methadone Addiction, Abuse, and Symptoms
TABLE OF CONTENTS
- I. The Basics
- II. Signs of Abuse
- III. Methadone Usage
- IV. How to Find Help
- V. Sources
The Basics
Methadone is also used in some cases as a prescription pain reliever. Clinicians also prescribe methadone as part of some addiction treatments. The Substance Abuse and Mental Health Services Administration notes that methadone is an option for medication-assisted treatment (MAT). This is because methadone reduces opioid withdrawal symptoms and cravings, making it more comfortable for someone working through the first critical days or weeks of rehab. Methadone also blocks some of the impacts of certain opioids, so the drugs become less of a temptation.
According to information published by the Anesthesia Patient Safety Foundation, methadone use is not without some risks. Safety alerts from the Federal Drug Administration indicate that the drug can impact the respiratory and cardiovascular systems. The risks seem to be more prevalent when someone is being treated for pain with high, regular doses of methadone. There’s also the risk that ongoing use of methadone for any reason — or misuse of it — can lead to addiction or overdose.
Primary Methadone Dangers
- Addictiveness: In 2007, Nutt et. al. conducted a comprehensive study regarding the addictive nature of various types of substances. One part of that study had independent experts weigh in on how addictive each drug actually was. Street methadone scored 2.8 on a scale of 3.0 when it came to dependence. Only heroin, cocaine, and tobacco were deemed more addictive.
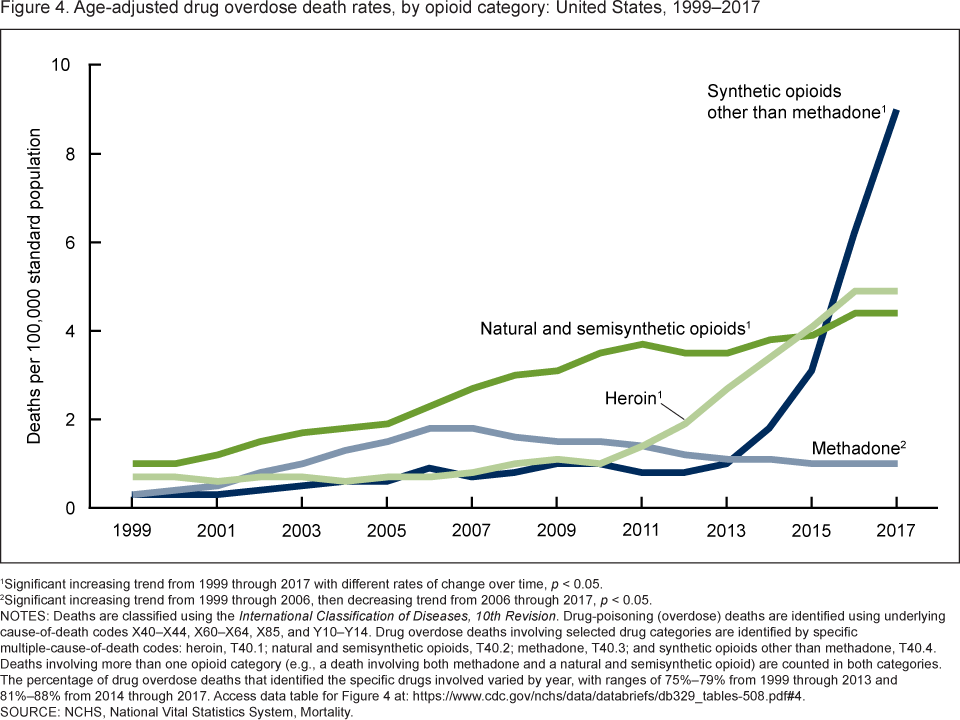
- Risk of overdose: Methadone is responsible for a disproportionate number of synthetic opioid deaths. The numbers are high enough that the CDC tracks them separately from deaths related to overdoses of other synthetic opioids. According to the CDC, the annual rate for deaths from an overdose related to methadone was 1 in every 100,000 people. Heroin, which is much more talked about within society, contributes to death by overdose rate of 5 in every 100,000 people.
- Unintended side effects: Methadone can cause side effects that include dry mouth, anxiety and nervousness, nausea, and drowsiness. More serious side effects can include hives, swelling of the tongue or facial area, increased heart rate, chest pain, hallucinations, and respiratory distress. Someone experiencing these types of side effects when taking methadone, prescribed or not, should seek medical help.
- Legal risks: Methadone is considered a Schedule II drug by the federal government. These are substances that have medical use but have a high risk of being abused. Non-medical trafficking of any amount of methadone can result in a prison sentence of up to 20 years. If someone is killed or seriously harmed by the drug use or sale, the sentence could be even higher. The person can also be fined up to $1 million. Second offenses come with even steeper legal penalties.
| Derived From | A synthetic opioid |
| Ways Used | Orally via a pill form, which can also be crushed for snorting or smoking or dissolved for injecting |
| Scientific Name | Methadone Hydrochloride |
| Slang/Street Names for Methadone | Street methadone, chocolate chip cookies, Maria, Salvia, Amidone, fizzes, wafer |
| How Long in Bodily System | Half-life: 24 hours
Elimination in a few days to two weeks, depending on factors such as use, age and health |
| Punitive Legal Measures: Using/Possession | Methadone is a Schedule II controlled substance. It’s illegal to have it or use it outside of a situation where you have a medical prescription. Illegal possession of methadone can lead to one or more years in prison. |
| Punitive Legal Measures: Selling/Distributing | Selling a Schedule II controlled substance comes with even more severe legal penalties. You can face up to 20 years in prison and a fine of up to $1 million for your first offense. |
| DEA Drug Rating | Schedule II |
Signs of Abuse
Behavioral Symptoms of Methadone Usage and Abuse
How methadone affects the brain
Methadone acts on the brain in the same way that many other opioids do. It changes the way your body reacts to pain, specifically causing your nervous system or brain to respond in a way that causes you to feel less pain. It also has a sedative effect, which means it can make you feel calm or sleepy. When taken in high doses, that sedative effect can turn into the euphoric high associated with other opioids.
However, methadone is different than other synthetic and natural opioids in a few ways. First, it tends to have a longer half-life. That means it, and its effects, stay in your system longer, which helps reduce withdrawal symptoms in someone who is trying to stop taking other opioids. Methadone also blocks the impact of other opioids, which means someone taking methadone as part of addiction treatment will find that heroin and other drugs don’t provide any type of high for them.
Behavioral signs of methadone usage and abuse
One of the biggest behavioral signs of methadone abuse is that the person has become physically dependent on the drug, and their actions are indicative of that dependence. They may have an increased tolerance, which means they need more methadone to achieve the same results — whether that’s pain relief or a high. They may also take uncharacteristic actions to gain possession of more of the drug, including lying, cheating, stealing, or engaging in risky behavior.
Other signs that someone may be struggling with methadone abuse or addiction include sudden and otherwise unexplained changes in behavior, eating and sleeping habits, mood, and overall health. Someone who is addicted will also experience withdrawal symptoms, which can range from depression and anxiety to muscle cramps and digestive issues.
Physical Symptoms of Methadone Abuse
How methadone affects the body
Methadone causes changes to the way your brain and nervous system work with the rest of your body. The results can be a sedation effect that helps relax you. In prescription situations, this may be used to provide relief for pain or other symptoms, but the drug can also be abused to achieve a euphoric high.
If you use too much methadone, it can result in other physical changes, including lower blood pressure and heart rate, tremors, diarrhea and vomiting, shallow breathing, confusion, and even coma. Since methadone has a longer half-life than many other opioids, all of these physical effects can last much longer than they might with a drug such as heroin. That makes methadone even more dangerous.
Early physical effects of methadone
Methadone starts working in your body shortly after the first dose. If taken in the proper dosage that adheres to a doctor’s prescription, the effects are usually pain relief and some relaxation. Abusing methadone can have both physical and psychological effects outside of the high that many people seek. The physical effects of methadone can be unpleasant and endanger your health.
This table illustrates the possible short-term physical effects associated with methadone.
| Short-Term Physical Symptoms | |
| Initial (direct effects of drug, 30 – 60 min.) | Sweating Runny nose Loss of appetite Yawning Aggression |
| Lingering (within an hour of taking the drug) | Headache Rashes and/or itching Difficulty passing urine Increased temperature Chills |
| Post-Use (several hours to days after use) | Joint or muscle aches Irritability and aggression Confusion Lethargy Craving for methadone Dependence (more likely in higher doses) Swelling in the arms or legs |
Severe and long-term physical effects of methadone
According to the American Society of Addiction Medicine, chronic use of methadone can result in a very serious addiction cycle. The withdrawal symptoms and cravings can be enough to drive many people back to use, and the ASAM even reports that some addiction treatment centers provide long-term medication-assisted programs where methadone is supplied to patients in low doses to stave off these issues.
In addition to a potentially difficult-to-beat addiction, methadone has some other long-term physical effects that are concerning. They range from annoying symptoms such as abdominal cramps to issues that might endanger health, such as cardiovascular issues, difficulty breathing, and memory loss.
This table illustrates the possible long-term physical effects associated with methadone.
| Long-Term Physical Symptoms | |
| Casual | Difficulty urinating Changes in sex drive Joint and muscle aches Digestive issues Changes in menstrual cycle |
| Chronic (Including all of the above effects for casual use) | Respiratory distress Cardiovascular issues Changes in blood pressure Reproductive issues Difficulty with memory or thought processes Difficulty with judgment and decision-making Changes in liver function Overdose and death |
| Withdrawal | Shaking Stomach issues, including cramps and diarrhea Irritability and anxiety Difficulty sleeping Runny nose Joint and muscle aches Restlessness |
Further Resources
Both the National Institute of Drug Abuse (NIDA) and the Substance Abuse and Mental Health Services Administration (SAMHSA) offer in-depth information on both the symptoms and treatment of prescription stimulant addiction.
Methadone Usage
Methadone use is a concern around the globe
According to the United Nations Office on Drugs and Crime, methadone is one of the main opioids misused in Europe. It’s also being abused in other nations, and the seizure of prescription opioids, in general, has risen significantly in recent years. In 2016, around 87 tons of prescription opioids were seized by law enforcement across the globe as part of drug trafficking and use investigations — that’s almost equal to the amount of heroin seized for the same time period.
In a single year, more than 50 million people across the globe will misuse opioids or opiates, according to the World Health Organization, and more than half of those individuals are likely struggling with an addiction to these drugs. WHO notes that around a third of all drug-related deaths are overdoses, and the vast majority of those cases are related to opioids, including methadone.
Opioid Use Throughout the World
| Highest | Second | Third | |
| Availability of prescription opioids | United States | Germany | Canada |
| Percent of adults using prescription opioids | United States | Australia | Czech Republic |
| Percent of adults using opioids of any type | United States | Australia | Afghanistan |
| Percent of adults using opiates of any type | Afghanistan | Seychelles | Iran |
Methadone Usage Demographics in the U.S.
The abuse of prescription drugs, particularly opioids, is a concern for people of all ages in the United States. The Monitoring the Future Survey doesn’t have data for prescription drug use for students below 12th grade, but, as of 2018, 15.5% of high school seniors said they had used prescription drugs outside of a doctor’s care at least once in their lifetime, and more than 4% had done so in the past month.
According to the National Institute on Drug Abuse, young adults — those ages 18 to 25 — abuse more prescription drugs than any other age group in the United States. They account for an average of five overdose deaths a day. A total of 46 people across all age groups die from an overdose daily, and around a third of those deaths are related to opioids. The CDC reports that methadone is the most common drug involved in these cases.
States with Highest Opioid Prescription Use and Death Rates
| Highest | Second | Third | |
| Opioid-involved overdose deaths | West Virginia | Ohio | New Hampshire |
| Opioid prescriptions | Tennessee | Oklahoma | Kentucky |
How to Find Help
Many times, methadone use begins with a prescription; however, prolonged use can lead to a tolerance for the medication. That means you need more of it to achieve the same results. Improper or long-term use of high doses of methadone can lead to addiction. At that point, individuals who stops using the drug may contend with uncomfortable or even dangerous withdrawal symptoms that drive them back to methadone use or even to abuse of other opioids.
Treating methadone abuse and addiction typically requires professional help. This is especially true when someone has become dependent on methadone during treatment for another addiction. To learn more about treatment options for methadone addiction and how to find help, read our methadone rehabilitation guide, which provides a comprehensive resource on this process.
Staging an Intervention
If you have a loved one who’s struggling with addiction, staging an intervention is often the first necessary step towards sobriety, but it’s important to be strategic and loving in your approach. Even the most well-meaning of interventions can have a negative effect if they aren’t handled correctly.
5 Tips for Staging an Intervention
| 1. Don’t Do It Alone. A professional interventionist is always the most qualified to guide a successful intervention. Also, rely on non-addict family and friends – especially those who have a close relationship with you or the addict. |
| 2. Research Ahead of Time. It’s best to do plenty of research ahead of time to gather insight on the addiction and how it affects the addict. Also, be prepared with local resources for getting help. |
| 3. Write Out Your Statement. During the actual intervention, emotions will likely be running high, so it’s best to have a statement of how the person’s addiction has impacted you and your relationship with him or her. These statements should be honest, yet written from a place of love – no personal attacks. |
| 4. Offer Help. It’s important for everyone attending the intervention to offer tangible help and support as the person works through detox and rehabilitation. |
| 5. Set Boundaries. If the person refuses to seek help and take the next steps outlined, it’s important that they understand that everyone present will end codependence and enabling behaviors. |
Sources
- https://books.google.com/books?id=HYPcBQAAQBAJ&printsec=frontcover&dq=Treatment+of+Opioid+dependence&hl=en&sa=X&ved=0ahUKEwjy0e7zl9fLAhUKMSYKHYh9At4Q6AEIRjAD
- https://data.unodc.org/
- https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/sma10-4120.pdf
- https://www.apsf.org/article/opioid-prescribing-methadone-risk-mitigation/
- https://www.asam.org/docs/default-source/practice-support/guidelines-and-consensus-docs/asam-national-practice-guideline-supplement.pdf
- https://www.camh.ca/-/media/files/guides-and-publications/straight-talk-methadone.pdf
- https://www.cdc.gov/opioids/basics/fentanyl.html
- https://www.cdc.gov/drugoverdose/deaths/prescription/maps.html
- https://www.cdc.gov/mmwr/volumes/66/wr/mm6612a2.htm
- https://www.cdc.gov/nchs/images/databriefs/301-350/db329_fig4.png
- https://www.dea.gov/drug-scheduling
- https://www.dea.gov/sites/default/files/drug_of_abuse.pdf
- https://www.drugabuse.gov/drugs-abuse/opioids/opioid-summaries-by-state
- https://www.drugabuse.gov/publications/drugfacts/prescription-opioids
- https://www.drugabuse.gov/drug-topics/trends-statistics/infographics/abuse-prescription-rx-drugs-affects-young-adults-most
- https://www.drugabuse.gov/sites/default/files/files/ClinicalOpiateWithdrawalScale.pdf
- https://www.drugabuse.gov/trends-statistics/monitoring-future/monitoring-future-study-trends-in-prevalence-various-drugs
- https://www.justice.gov/archive/ndic/pubs6/6096/index.htm
- https://nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Methadone%C2%AE
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3171821/
- https://www.oecd.org/els/health-systems/opioids.htm
- https://www.samhsa.gov/homelessness-programs-resources/hpr-resources/teen-prescription-drug-misuse-abuse
- https://www.samhsa.gov/medication-assisted-treatment/treatment/methadone
- https://www.thelancet.com/action/showPdf?pii=S0140-6736%2807%2960464-4
- https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_3_DRUG_MARKETS.pdf
- https://www.who.int/substance_abuse/information-sheet/en/
{kind=link}